Cervical Vertebrae Synostosis & Its Clinical Significance
Singh B.1, Gautam P.2, Gupta S.3*
1 Bindu Singh, Assistant Professor, Department Of Anatomy, BRD Medical college, Gorakhpur, Uttar Pradesh, India.
2 Prateek Gautam, Lecturer, Department Of Anatomy, BRD Medical college, Gorakhpur, Uttar Pradesh, India.
3* Shalini Gupta, Department Of Anatomy, BRD Medical college, Gorakhpur, Uttar Pradesh, India.
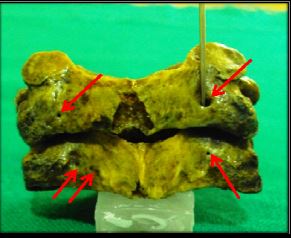
Normal typical cervical vertebrae are characterized by the presence of smaller body, foramina transversarium, triangular spinal canal. The superior articular facet are directed in upward & backward direction while the, inferior articular facet are directed forward & downwards and has a short bifid spine. Abnormalities in any of the features may be associated with neurological signs and symptoms. During the routine osteology classes we found two abnormally fused typical cervical vertebrae in the Department of anatomy, BRD medical college, Gorakhpur. These abnormalities may lead to significant sign and symptoms thus this case is being studied
Keywords: Body, Extra Foramina, Facets, Fused Cervical Vertebrae
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department Of Anatomy, BRD Medical college, Gorakhpur, Uttar Pradesh, India. Email:  |
Bindu Singh, Prateek Gautam, Shalini Gupta, Cervical Vertebrae Synostosis & Its Clinical Significance. Biomed Rev J Basic Appl Med Sci. 2014;1(2):49-52. Available From https://www.biomedicalreview.in/cervical-vertebre-synostosis-its-clinical-significance-case-report |
 |
 ©
© 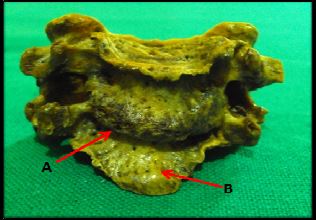 Fig 1: Arrows [A] showing complete fusion of body & [B] protrusion of lower border of lower cervical vertebrae
Fig 1: Arrows [A] showing complete fusion of body & [B] protrusion of lower border of lower cervical vertebrae