A Study on risk factors and Microbial profile of Ventilator associated Pneumonia in Intensive care units of a Tertiary care centre
Shetty S.1, Kiran V.2*, Bhat R.3, Alam N.4
1 Sanmath K Shetty, Junior resident, Department of Internal medicine, KMC, Mangalore, Karnataka, India.
2* VH Kiran, Junior resident, Department of Internal medicine, KMC, Mangalore, Karnataka, India.
3 Raghavendra V Bhat, Professor and HOD, Department of Internal medicine, KMC, Mangalore, Karnataka, India.
4 Nawaz Alam, Associate Professor, Department of Internal medicine, KMC, Mangalore, Karnataka, India.
Background: Ventilator associated pneumonia is a major cause of in hospital mortality and morbidity in our ICUs and it has received more importance with the advent of drug resistance. The knowledge of local antibiotic susceptibility patterns would guide the physician in the early empirical treatment of VAP. Our aim was to know the risk factors and microbial profile of Ventilator Associated Pneumonia patients. Methodology: We randomly studied 120 patients on ventilator in the 3 ICUs of KMC, Mangalore. VAP was diagnosed according to the case definition of VAP. The risk factors were analyzed and microbiological profile of patients who developed VAP was studied. Results: OF the 120 patients, 59 developed VAP. Prolonged ventilation and reintubation were the risk factors most significantly associated with the development of VAP. Gram negative organisms (acinetobacter, pseudomonas, klebsiella) were the most commonly isolated organisms from specimens of VAP cases and there was high prevalence of multidrug resistance. Carbapenem resistant Acinetobacter baumanii was an important pathogen in the ICU of University Medical Centre Mangalore. Vancomycin was sensitive against most gram positive isolates whereas amikacin and cefaperazone sulbactum was showing acceptable sensitivity to gram negative isolates except for Acinetobacter species. Colistin may be useful as a rescue antibiotic in carbapenem resistant Acinetobacter VAP. Conclusion: Incidence of VAP is directly proportional to duration of mechanical ventilation and Reintubation is a strong risk factor for development of VAP. Therefore, administering a proper weaning protocol and titrating sedation regimens as per the need of the patients is of utmost importance
Keywords: Pneumonia, Ventilator, Intensive care units, Drug resistance
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior resident, Department of Internal medicine, KMC, Mangalore, Karnataka, India. Email:  |
Sanmath K Shetty, VH Kiran, Raghavendra V Bhat, Nawaz Alam, A Study on risk factors and Microbial profile of Ventilator associated Pneumonia in Intensive care units of a Tertiary care centre. Biomed Rev J Basic Appl Med Sci. 2015;2(2):53-58. Available From https://www.biomedicalreview.in/risk-factors-microbial-profile-ventilator-associated-pneumoni-intensive-care-units-research-article |
 |
 ©
© 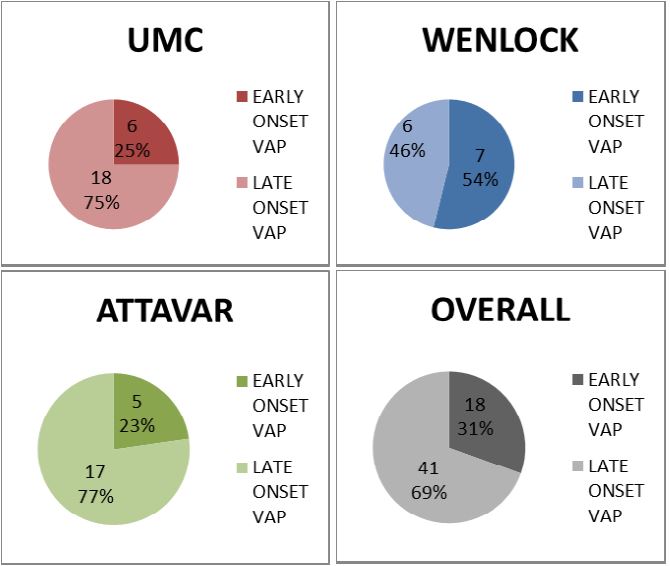
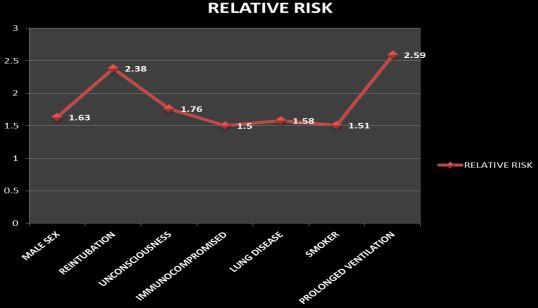
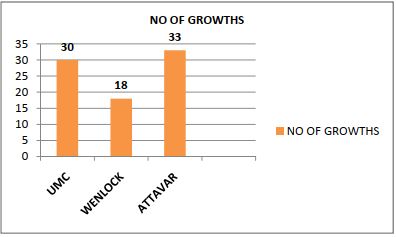 Fig 3: Isolates from 3 ICUs
Fig 3: Isolates from 3 ICUs