Incidence of spontaneous Intracranial Hemorrhage( ICH) & utility of the ICH scores in stroke patients
Grace M.1*, Jacob K.2, Shameer V.3, Sudhiraj.4, Vijayan S.5, Das R.6, Sasindran S.7
1* Mary Grace, Associate Professor, Department of Medicine, Government Medical College, Thrissur, Kerala, India.
2 K J Jacob, Additional Professor, Department of O & G, Government Medical College, Thrissur, Kerala, India.
3 V K Shameer, Assistant Professor, Department of Medicine, Government Medical College, Kozhikode, Kerala, India.
4 Sudhiraj, Assistant Professor, Department of Community Medicine, Government Medical College, Thrissur, Kerala, India.
5 Sarang Vijayan, Senior Resident, Department of Medicine, Government Medical College, Thrissur, Kerala, India.
6 Remya Das, Senior Resident, Department of Medicine, Government Medical College, Thrissur, Kerala, India.
7 Sooraj Sasindran, Junior Resident, Department of Medicine, Government Medical College, Thrissur, Kerala, India.
Introduction: The aim of the study was to find out the incidence of spontaneous ICH in patients hospitalized with stroke, to study the predictive value of clinical and radiological findings in determining the mortality and short term outcome and to study the utility of the ICH scores. Materials and Methods: Among the 348 consecutive patients admitted with stroke, those who were diagnosed to have primary ICH, were included in the study. The mortality and outcome were predicted using the ICH scores. Data was analyzed using SPSS software and epi info. Results: Of the 130 cases with hemorrhage there were 102 patients (29.31%) with spontaneous ICH. The cut off value of the intracerebral bleed in relation to mortality was calculated as 22.5 ml. At the end of three months 100 people were available for follow up, only 9 (21.9%) were physically dependant on others for their living. All the three ICH scores were found to be statistically significant in predicting mortality at one month, but they did not fare well in predicting the short term outcome. Conclusion: We have observed an increased incidence of hemorrhagic stroke among hospitalized patients with stroke,(29%) when compared to western studies. Volume of the hemorrhage more than 22.5 ml was associated with poor prognosis .We observed a significant improvement in the functional status at three months, with 31% of the survivors able to lead independent lives. All the three ICH scores did not fare well in predicting the short term outcome.
Keywords: Intracerebral Hemorrhage, ICH score, Mortality, Short Term Outcome
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Medicine, Government Medical College, Thrissur, Kerala, India. Email:  |
Mary Grace, K J Jacob, V K Shameer, Sudhiraj, Sarang Vijayan, Remya Das, Sooraj Sasindran, Incidence of spontaneous Intracranial Hemorrhage( ICH) & utility of the ICH scores in stroke patients. Biomed Rev J Basic Appl Med Sci. 2015;2(3):68-74. Available From https://www.biomedicalreview.in/incidence-spontaneous-intracranial-hemorrhage-ich-utility-ich-scores-stroke-research-article |
 |
 ©
© 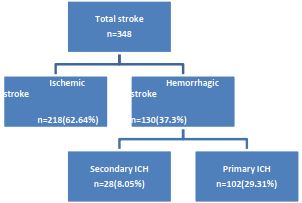
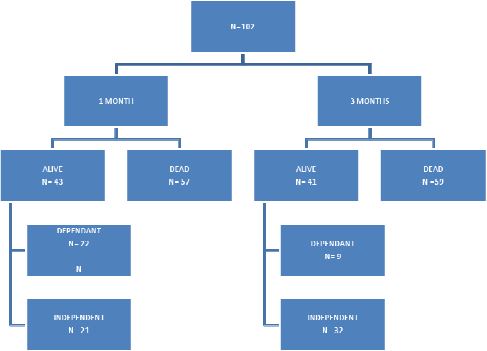
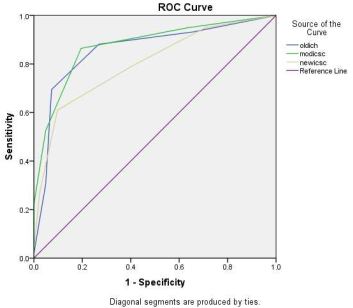 Figure 3: ROC curve comparing the ICH scores in predicting one month mortality
Figure 3: ROC curve comparing the ICH scores in predicting one month mortality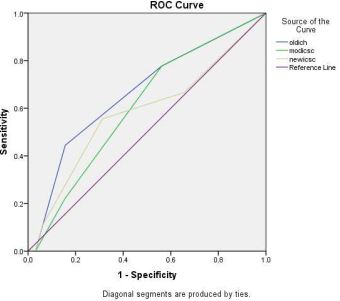 Figure 4: ROC curve of the ICH scores in predicting short term outcome
Figure 4: ROC curve of the ICH scores in predicting short term outcome