Determining the role of intra-uterine contraceptive device, oral contraceptive pills and multiple sexual partners in altered vaginal flora leading to bacterial vaginosis, in patients attending a tertiary care hospital in central Maharashtra, India
Rangari A.1*, Vashisth R.2
1* Amit A. Rangari, Associate Professor, Department of Microbiology, Muzaffarnagar Medical College and Hospital, Muzaffarnagar, U.P, India.
2 Ravi Vashisth, Tutor, Department of Microbiology, Muzaffarnagar Medical College and Hospital, Muzaffarnagar, U.P, India.
Background and Objective: Risk Factors of Bacterial Vaginosis (BV) includes multiple sex partners, sex without a condom, douching (washing the inside of vagina with a stream of water),poor hygiene, use of sexual toys or aids without proper cleaning, using an intrauterine device (IUD) for contraception. The precise contribution of sexual transmission to the overall epidemiology of the condition remains controversial. This study was undertaken with a objective to find out the role and association of risk factors like Intra-uterine contraceptive device (IUCD), Oral contraceptive pills(OCP’s), Multiple Sexual Partners in alteration of normal vaginal flora leading to BV. Material and Methods: High Vaginal Swabs of two hundred and fifty women of reproductive age (15 – 45 years) group who attended Gynaecology and Obstetrics OPD/IPD at tertiary care hospitals formed the study population. Detail patient history was noted. Nugent score elicited. Results: Bacterial Vaginosis was more in women using IUCD i.e. 77% (17) cases as compared to women using OCP i.e. 21 % (3) cases and to women not using OCP/IUCD i.e. 12% (8) cases. Bacterial vaginosis was more in women with abnormal sexual behaviour, with multiple partners i.e. prevalence was 50% (4/8 cases) as compared to women with normal sexual behaviour, with one male partner i.e. prevalence was 31.2 % (75/240cases) and in virgins prevalence of BV was 0 %( 0/2cases). Conclusion: Bacterial vaginosis is associated with sexual activity like multiple sexual partner, douching, intrauterine-device and oral contraceptives.
Keywords: Bacterial vaginosis, Intra-Uterine Contraceptive Device, Multiple Sexual Partners, Oral Contraceptive Pills
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Microbiology, Muzaffarnagar Medical College and Hospital, Muzaffarnagar, U.P, India. Email:  |
Amit A. Rangari, Ravi Vashisth, Determining the role of intra-uterine contraceptive device, oral contraceptive pills and multiple sexual partners in altered vaginal flora leading to bacterial vaginosis, in patients attending a tertiary care hospital in central Maharashtra, India. Biomed Rev J Basic Appl Med Sci. 2015;2(3):79-84. Available From https://www.biomedicalreview.in/intra-uterine-contraceptive-device-oral-contraceptive-pill-multiple-sexual-partners-research-article |
 |
 ©
© 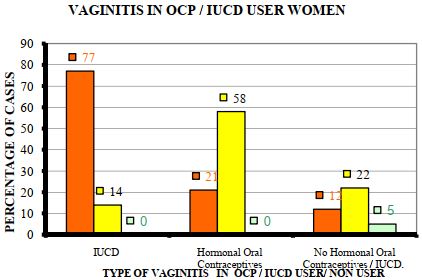
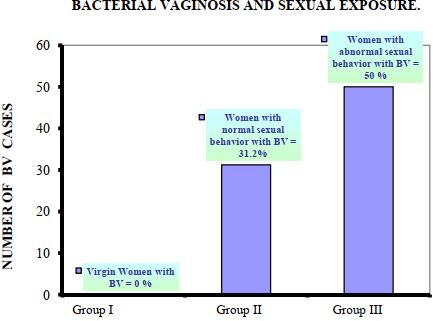 Figure 2:- Coexistence observed between bacterial vaginosis and sexual exposure.
Figure 2:- Coexistence observed between bacterial vaginosis and sexual exposure.