Pattern of medications prescribed for URI (upper respiratory tract infection) patients in medicine OPD of tertiary care teaching hospital, Ujjain
Mehta M.1*, banode S.2, Chourishi A.3
1* Maulin Mehta, Assistant Professor, Department of Pharmacology, RD Gardi Medical College, Ujjain, Madhya Pradesh, India.
2 Siddharth banode, Assistant Professor, Department of Pharmacology, RD Gardi Medical College, Ujjain, Madhya Pradesh, India.
3 Ashutosh Chourishi, Professor & Head, Department of Pharmacology, RD Gardi Medical College, Ujjain, Madhya Pradesh, India.
Objective: To obtain information on prescribing pattern of medications for URTI and comment on its effectiveness. Materials and Method: This observational, non-interventional and prospective study was carried out on patients with URTI, >18 years of age and of either sex came to medicine OPD over a period of 3 months. All the relevant information related with prescribed medications were recorded in annexure. Data obtained from the study were entered in MS Excel 2007 and analyzed. Result: Most common diagnosis was non specific URTI (50%), in total 96 prescriptions. Total 255 drugs were prescribed with average number of drugs per encounter were 2.65. Total percentages of encounters with antibiotic prescribed were 47.91%. Total numbers of FDCs prescribed were 10.38%, which include terbutaline+ambroxol (62.50%), amoxicillin+clavulanic acid (33.34%) and ampicillin+cloxacillin (4.16%). Total 47 antibiotics were prescribed, which were amoxicillin (28), amoxicillin+ clavulanic acid (9), azithromycin (9) and ampicillin+ cloxacillin (1). Out of total 255 drugs, antihistamines (27%, cetirizine) were prescribed for maximum number of time, followed by demulcents (20.24%, linctus syrup), antibiotics (19.02%), NSAIDS (18.21 %, paracetamol), bronchodilator (6.07%, terbutaline), mucolytic (6.07%, ambroxol) and antacids (3.23%, ranitidine). Conclusion: Proper and effective prescribing pattern of medications, for any condition, is required to improve drug efficacy, decrease cost of therapy, adverse effects, drug-drug interaction and drug resistance
Keywords: Polypharmacy, Antibiotic resistance, FDCs (Fixed Dose Combinations), Antihistamines
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Pharmacology, RD Gardi Medical College, Ujjain, Madhya Pradesh, India. Email:  |
Maulin Mehta, Siddharth banode, Ashutosh Chourishi, Pattern of medications prescribed for URI (upper respiratory tract infection) patients in medicine OPD of tertiary care teaching hospital, Ujjain. Biomed Rev J Basic Appl Med Sci. 2015;2(4):113-117. Available From https://www.biomedicalreview.in/pattern-medications-prescribed-uri-upper-respiratory-tract-infection-medicine-research-article |
 |
 ©
© 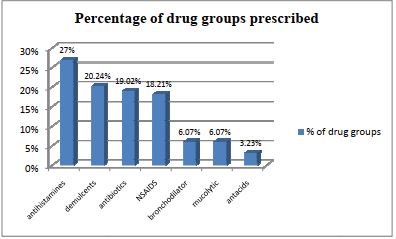 Figure-І: Different drug groups among prescribed drugs
Figure-І: Different drug groups among prescribed drugs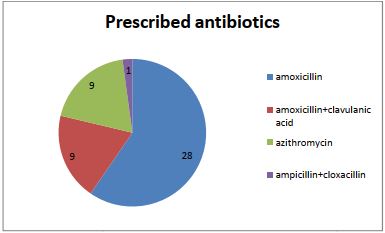 Figure ІІ: Distribution of prescribed antibiotics
Figure ІІ: Distribution of prescribed antibiotics