Mucocele of appendix in an elderly male from tuberculosis endemic region
Khadanga S.1*, Dugar D.2, Khurana U.3, Thatoi P.4, satapathy S.5
1* Sagar Khadanga, Assistant Professor, Department of Medicine, AIIMS, Bhopal, Madhya Pradesh, India.
2 Dharmendra Dugar, Assistant Professor, Department of Surgery, Hitech Medical College, Bhubaneswar, Odisha, India.
3 Ujjawal Khurana, Assistant Professor, Department of pathology, People’s College of Medical Sciences, Bhopal, Madhya Pradesh, India.
4 Pravat Kumar Thatoi, Assistant Professor, Department of Medicine, SCB medical college, Cuttack, Odisha, India.
5 Shakti Prasad satapathy, Senior consultant, Department of Medicine, Aditya care hospital, Bhubaneswar, Odisha, India.
A 55 year old gentleman with past history of pulmonary tuberculosis 6 years back presented with diffuse abdominal pain associated with fever, vomiting and a vaguely palpable mass in right iliac fossa. Ultrasonography showed distended ileal loops in the right lower quadrant of abdomen. CT scan abdomen revealed thickened, enlarged and fluid filled appendix suggestive of mucocele. Laparoscopy revealed approximately 22cm X 5cm mucocele of appendix with omental adhesions. Laparoscopic appendectomy was done, without any spillage of mucin in the peritoneum. The patient was discharged from the hospital on 3rd postoperative day and on ten months of follow up the patient is doing well. Laparoscopic appendectomy do not increase complication rate in mucocele of appendix
Keywords: Mucocele of appendix, Mucinous cystadenoma, Pseudomyxomaperitonei
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Medicine, AIIMS, Bhopal, Madhya Pradesh, India. Email:  |
Sagar Khadanga, Dharmendra Dugar, Ujjawal Khurana, Pravat Kumar Thatoi, Shakti Prasad satapathy, Mucocele of appendix in an elderly male from tuberculosis endemic region. Biomed Rev J Basic Appl Med Sci. 2016;3(1):153-155. Available From https://www.biomedicalreview.in/mucocele-of-appendix-in-an-elderly-male-from-tuberculosis-endemic-region-case-report |
 |
 ©
© 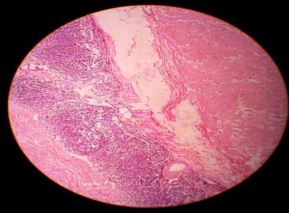 Fig 1: Intra operative image of laparoscopic appendectomy for mucocele.
Fig 1: Intra operative image of laparoscopic appendectomy for mucocele. Fig-2: Cut specimen of appendix showing mucin.
Fig-2: Cut specimen of appendix showing mucin. Fig 3: Histopathology showing appendix wall lined with mucinous epithelium.
Fig 3: Histopathology showing appendix wall lined with mucinous epithelium.