Effectiveness of auditory and visual cues on Bradykinesia in individuals with Parkinson’s disease: a comparative study
Joshi S.1*, Deshpande A.2
1* Snehal Joshi, Professor, D.E. Society’s Brijlal Jindal College of Physiotherapy, Pune, Maharashtra, India.
2 Arohi Deshpande, Intern, D.E. Society’s Brijlal Jindal College of Physiotherapy, Pune, Maharashtra, India.
Introduction: Parkinson’s disease (PD) is a neurodegenerative disorder affecting the physical, psychological, social, and functional status of an individual. Individuals with Parkinson’s disease (PD) often demonstrate bradykinesia during mobility tasks. Due to bradykinesia; a person with Parkinson’s may have difficulty performing everyday functions. This leads to activity limitation and participation restriction in these individuals. Hence different strategies are needed to overcome bradykinesia. Use of visual cues and auditory cues can be thought of improving this problem. Hence this study was conducted to find out the efficacy of auditory cues and visual cues and compare them. Objectives 1)To assess the effectiveness of auditory cues on bradykinesia in Parkinson’s patients 2) To assess the effectiveness of visual cues on bradykinesia in Parkinson’s patients. 3) To compare the effectiveness of auditory and visual cues on bradykinesia in Parkinson’s patients. Methodology: After obtaining consent from the subjects, they were randomly divided into 3 groups in where they received either auditory cues (Metronome beats) or visual cues (video) or no cues for the selected functional activities. Reaction time was measured before and after intervention. Conclusion: It was concluded that auditory cues are effective in improving bradykinesia
Keywords: Auditory cues, Bradykinesia, Parkinson’s disease, Visual cues
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, , D.E. Society’s Brijlal Jindal College of Physiotherapy, Pune, Maharashtra, India. Email:  |
Snehal Joshi, Arohi Deshpande, Effectiveness of auditory and visual cues on Bradykinesia in individuals with Parkinson’s disease: a comparative study. Biomed Rev J Basic Appl Med Sci. 2017;4(1):190-196. Available From https://www.biomedicalreview.in/effectiveness-auditory-visual-cues-bradykinesi-individuals-parkinson-s-disease-research-article |
 |
 ©
©  Graph-I: Shows gender wise distribution of the subjects
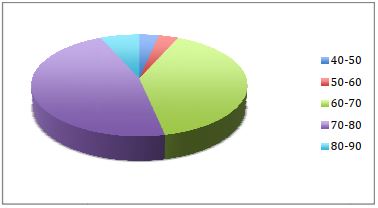
Graph-I: Shows gender wise distribution of the subjects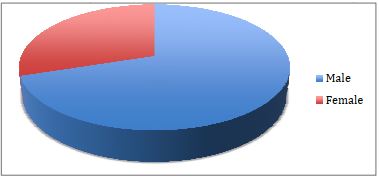 Graph-II: Shows age wise distribution of the subjects
Graph-II: Shows age wise distribution of the subjects