Effectiveness of Stretching on Kinesiophobia and Health-related Quality of Life in Quarry Workers with Work-related Low Back Pain
Bolarinde S.1*, Adegoke B.2, Ayanniyi O.3, Olagbegi M.4
1* Samuel Olufemi Bolarinde, Department of Physiotherapy, Federal Medical Centre, Owo, Ondo, Nigeria.
2 Babatunde O A Adegoke, Professor, Department of Physiotherapy, College of Medicine, University of Ibadan, Oyo, Nigeria.
3 Olusola O Ayanniyi, Senior Lecturer, Department of Physiotherapy, College of Medicine, University of Ibadan, Oyo, Nigeria.
4 Michael O Olagbegi, Department of Physiotherapy, Federal medical Centre, Owo, Ondo, Nigeria.
Introduction: The study was designed to compare the effectiveness of eight-week stretching exercise combined with back care education, lumbar stabilization combined with back care education and back care education on kinesiophobia and health-related quality of life in quarry workers with work-related low back pain (WRLBP). Materials and Methods: The randomized clinical trial involved 96 quarry workers with WRLBP randomly assigned into Stretching Exercise with Back Care Education Group (SEBCEG), Lumbar Stabilisation Exercise with Back Care Education Group (LSEBCEG) and Back Care Education Group (BCEG). Participants kinesiophobia was assessed using Tampa scale of kinesiophobia while health- related quality of life was assessed using WHO health-related quality of life. Participants were treated twice weekly and evaluated at baseline, week 4 and week 8 of the study. Data were analysed using descriptive statistics, ANOVA, Friedman’s ANOVA and Kruskal-Wallis test at α 0.05. Results: Eighty – six participants completed the study with no significant differences in demographic and clinical characteristics between the three groups at baseline. Participants in the SEBCEG demonstrated more significant reductions (p < 0.05) in kinesiophobia and more improvement in quality of life than those in both LSEBCEG and BCEG at the end of week 8 of the study. There were significant within-group improvements (p < 0.05) in all variables for the three groups thus indicating the effectiveness of each intervention. Conclusion: Stretching exercises are better than lumbar stabilisation exercises and back care education in reducing kinesiophobia and improving health-related quality of life pain in individuals with WRLBP
Keywords: Kinesiophobia, quality of life, Stretching exercises, Work-related low back pain
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department of Physiotherapy, Federal Medical Centre, Owo, Ondo, Nigeria. Email:  |
Samuel Olufemi Bolarinde, Babatunde O A Adegoke, Olusola O Ayanniyi, Michael O Olagbegi, Effectiveness of Stretching on Kinesiophobia and Health-related Quality of Life in Quarry Workers with Work-related Low Back Pain. Biomed Rev J Basic Appl Med Sci. 2017;4(1):197-205. Available From https://www.biomedicalreview.in/stretching-kinesiophobi-health-life-quarry-workers-work-related-low-back-pain-research-article |
 |
 ©
© 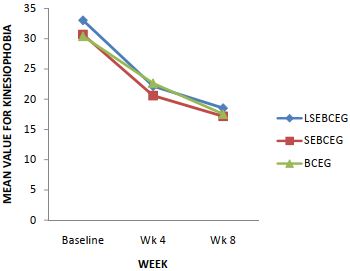 Figure-1: Trends of kinesiophobia pain for the LSEBCEG, SEBCEG and BCEG at the three time points of the study
Figure-1: Trends of kinesiophobia pain for the LSEBCEG, SEBCEG and BCEG at the three time points of the study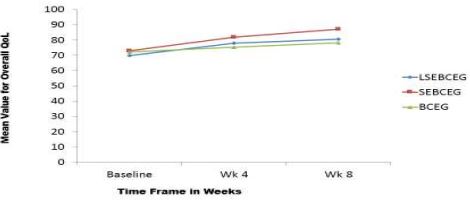 Figure-2: Trends of QoL overall for the LSEBCEG, SEBCEG and BCEG at the three time points of the study.
Figure-2: Trends of QoL overall for the LSEBCEG, SEBCEG and BCEG at the three time points of the study.