

Introduction
Respiratory Syncytial virus (RSV) is one of the leading causes of bronchiolitis and pneumonia in hospitalised infants and young children (1,2). Co-infections of RSV A/B with other respiratory pathogens in paediatric ARTI (acute respiratory tract infections) are frequent but the diagnostic significance, clinical severity, and outcomes of coinfections are conflicting. Few studies document low severity while others have a severe presentation (3,4). The BioFire FilmArray Respiratory Panel enables simultaneous detection of several respiratory viral pathogens and has been employed in this study, carried out at Kanchi Kamakoti Childs Trust Hospital (KKCTH), a paediatric hospital in Chennai, from 2016-2018 to assess the incidence and clinical severity of RSV single and co-infections in hospitalised children with ARTI.
Methodology
The Kanchi Kamakoti CHILDS Trust Hospital ethics committee (KKCTH/CTMRF/EC/VERI STUDY letter dated 21/07/2016 approved this study. After the Informed consent process, screened subjects were enrolled after meeting the inclusion criteria. A single-time nasopharyngeal swab was taken and stored at -80 degrees Celsius and PCR was analysed. Subject’s demographics, clinical symptoms, vitals, vaccine status and follow-up data were captured in case report form. All the data were entered into an MS Excel sheet and coded for statistical analysis.
Results
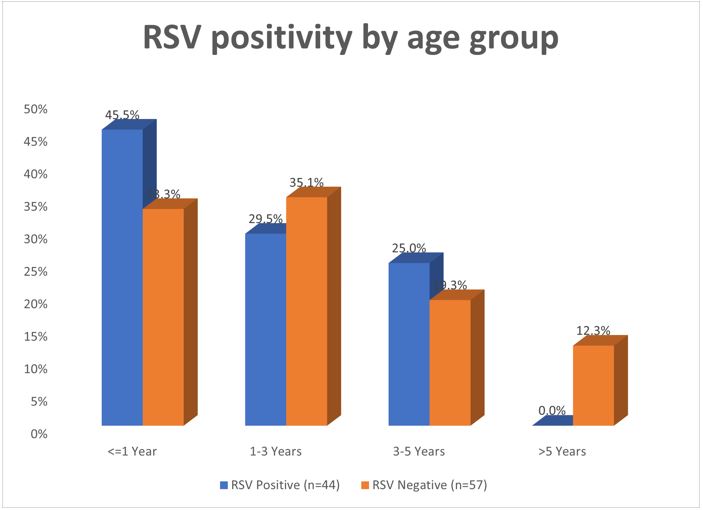
101 subjects were recruited; the ratio of males to females was 1.7:1. The most prevalent respiratory pathogens were RSV (25.7%) human bocavirus (10.8%), rhinovirus (4.9%) and human metapneumovirus (3.9%). RSV A and B were detected in both single and co-infections. RSV A/B caused single (n=13, 12.8%) and mixed/co-infections (n=10, 9.9%). Age-based analysis indicated that the brunt of RSV infections was borne by those up to 1 year of age with 45.5% positivity compared to 29.5% in children >1 to 3 years and 25% in those >3 and 5 years. Mean age of RSV cases was 1.73 years compared to 2.62 years of RSV negative cases. Fever (97.7%) and cough (100%), wheeze (86.4%) and difficulty in breathing (75%) were the common clinical manifestation amongst RSV cases. Decreased feeding was significantly associated (p=0.044) with RSV cases. There was no significant difference between the clinical severity of single or mixed RSV infections. Lethargy was significantly associated with RSV mixed infections (p=0.037) while oxygen support was significantly higher in single RSV infections (p=0.021). The average days of hospitalisation of those with single and mixed RSV infection were 5.55 and 2.5 days respectively. Significantly, RSV A/B infections (n=21, 91%) coincided with the onset of the month during September and October. The presence of a smoker in the household was significantly associated with RSV infection (40.9%; p=0.001) and the odds of RSV infection were 5.89 times (95% CI: 2.09 – 16.61) higher in the smoking environment.
Discussion and Conclusion
RSV causes significant ARTI in children between 6 months to 1 year possibly due to waning of maternal neutralizing RSV antibodies. Co-infections of RSV with other viral pathogens are common in paediatric ARTI yet they are not significantly different from single infections regarding severity, clinical outcome and patient management (5,6). Greater oxygen support and longer hospitalisation were observed in single RSV infections. BioFire Respiratory Panel provides early results which affects better clinical management and outcome (2). The role of human bocavirus and metapneumovirus in paediatric ARTI needs further research (7,8). The maternal RSV vaccine of Pfizer launched in 2023 projects a substantial reduction in severe RSV disease in newborns and infants up to 6 months of age. An effective vaccine for immunization of young infants and children is the need of the hour.
Acknowledgements: We acknowledge the contribution of King Institute, Guindy towards the study.
References
1. Wang X, Li Y, O'Brien KL, Madhi SA, Widdowson MA, Byass P, et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: a systematic review and modelling study. Lancet Glob Health. 2020;8(4):e497-e510. doi:10.1016/S2214-109X(19)30545-5 [Crossref][PubMed][Google Scholar]
2. Vos LM, Bruning AHL, Reitsma JB, Schuurman R, Riezebos-Brilman A, Hoepelman AIM, et al. Rapid Molecular Tests for Influenza, Respiratory Syncytial Virus, and Other Respiratory Viruses: A Systematic Review of Diagnostic Accuracy and Clinical Impact Studies. Clin Infect Dis. 2019;69(7):1243-1253. doi:10.1093/cid/ciz056 [Crossref][PubMed][Google Scholar]
3. Rogers BB, Shankar P, Jerris RC, Kotzbauer D, Anderson EJ, Watson JR, et al. Impact of a rapid respiratory panel test on patient outcomes. Arch Pathol Lab Med. 2015;139(5):636-641. doi:10.5858/arpa.2014-0257-OA [Crossref][PubMed][Google Scholar]