Introduction
Background
The pre-admission pre-anesthesia evaluation clinic is a site where patients are assessed prior to ward admission for a scheduled surgical procedure [1]. This helps to create a record of documentation from patient history and physical examination, and to deliver quality patient care through risk assessment, optimization, perioperative management, and final decisions[2]. Pre-anesthesia evaluation is an activity or practical approach that opens the way for the provision of anesthetic care for surgical procedures[3].
PAAE involves an interview and general physical examination; reviewing of prior of medicine history, surgery, and anesthesia related concerns; present or previous drug usage; and a review of prerequisites to obtain and review important finding before surgery[4]. An anesthetist or Anesthesiologist conduct pre-admission anesthesia assessment at anesthesia clinic[5]. In terms of reducing anxiety, pre-admission anesthesia clinical assessment is more successful than pre-anesthetic assessment ward[6].
PAE clinics permit increased communication between anesthesia providers and initial patient encounters with anesthetists, allowing better preoperative counseling, involving anesthetist in developing practical guidelines, and coordination of patient care following surgery to decrease pain, postoperative complications, hospital stay, and death [7].
Anesthetist or Anesthesiologist‑directed pre-admission anesthesia evaluation at the pre-admission clinic for preoperative evaluation have shown that the clinical practice approach reduce patient cancellations on the day of surgery because of poor preparation prior to surgery [7].
A pre-admission anesthesia evaluation is conducted to assess the overall medical conditions and risks of patients, and to recommend and develop a plan for management and anesthesia [8]. Hence, pre-admission anesthesia evaluation is part of anesthesia practice [9].
To obtain a detailed medical and anesthetic history and appropriate physical examination, all outpatient surgical patients must undergo pre-admission anesthesia evaluation and consultation [10]. Pre-admission evaluation assesses patient's general status and other related medical conditions [5].
Proper documentation of a pre-admission anesthesia chart was necessary as to the standard clinical practice guideline described by the South African Society of Anesthesiologists in 2012 [1]. A significant shortcoming in improving postoperative patient outcomes is inadequate or partial reporting of the patient's preoperative state [11].
The pre-admission anesthesia evaluation record, electronic or handwritten, compiles conditions of every patient’s pre-admission status, including pre-anesthetic care recommendations [12]. This enables essential pre-anesthetic planning [13]. Accurate data collection for anesthetic record of assessed patient is crucial for improving quality of clinical care based on information generated from necessary documents [7].
Proper recording of patient data is a crucial part of clinical practice [14]. This might related to improvement of overall quality of clinical care and permit an easy way of handling and handover of patient data among health professionals [2]. Recording the patient data at the pre-admission anesthetic evaluation should be kept or attached in the patient’s medical card; Which is essential for medico legal purposes and quality assurance [15][16]. However, poor chart recording and documentation at the pre-admission anesthesia clinics are considered as an avoidable obstacles affecting the quality of clinical care and patient outcomes [17][18].
Moreover, the American Society of Anesthesiologists (ASA) ethics guideline recommend that the anesthetists or anesthesiologists play a great role in the provision of pre-anesthetic evaluation and assessment for their clients on the ethical basis of anesthesia practice [19].
Significance of the audit
The purpose of this audit was to increase the practice of record keeping at a pre-admission anesthesia clinic among anesthesia professionals at HUCSH. This audit aimed to provide excellent practice, an area that hinders the practice of good documentation in anesthesia clinics and needs to be improved. Filling this gap can improve the quality and safety of patient care and reduce mortality and morbidity. In addition, this audit guards patients from an economic burden by reducing cancellations on the day of surgery. Hence, we were aimed to assess the utilization of proper recording at pre-anesthesia clinics based on these guidelines.
Aim of the study
This study aimed to promote best available current evidence-based practice of documentation at pre-admission anesthesia clinics among anesthesia professionals for outpatient surgical patients at Hawassa University Comprehensive Specialized Hospital in 2023.
Objectives of the audit
General Objective:
- To assess the practice of documentation at the pre-admission anesthesia clinic and provide best available evidence-based practice among anesthesia professionals for outpatient surgical patients at HUCSH in 2023.
Specific Objectives:
- To determine the practice of documentation at the pre-admission anesthesia clinic among anesthesia professionals for outpatient surgical patients at HUCSH in 2023.
- To provide best available evidence-based practice among anesthesia professionals for outpatient surgical patients at HUCSH in 2023.
- To identify areas of practice of documentation at a pre-admission anesthesia clinic that need improvement among anesthesia professionals for outpatient surgical patients at HUCSH in 2023.
- To reflect on baseline reporting of practice of documentation at a pre-admission anesthesia clinic among anesthesia for outpatient surgical patients at HUCSH in 2023.
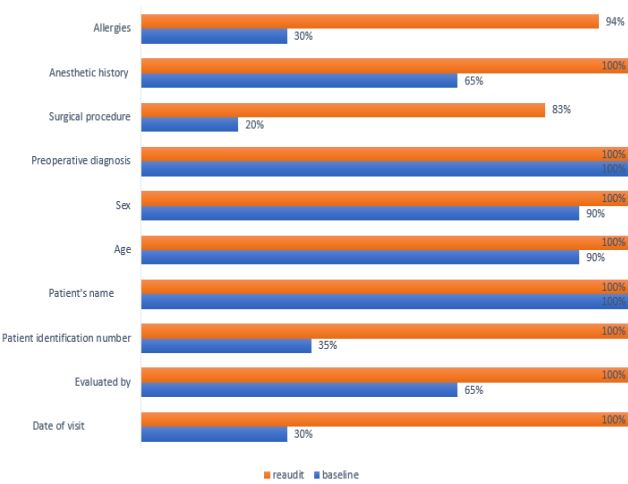
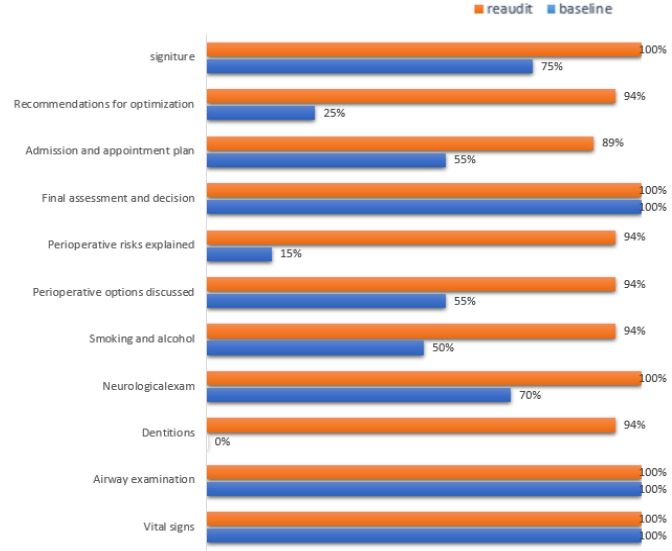
 Figure–1a: The practice of documentation at the pre-admission anesthesia clinic among anesthesia professionals for outpatient surgical patients at Hawassa University Comprehensive Specialized Hospital, 2023.
Figure–1a: The practice of documentation at the pre-admission anesthesia clinic among anesthesia professionals for outpatient surgical patients at Hawassa University Comprehensive Specialized Hospital, 2023.