Introduction
Interdisciplinary cohesion is indispensable in patient management. Exchange of scientific information between the various specialties of medicine paves the way forward to productive patient outcomes. We share an example of interdisciplinary cohesion in the management of a patient with parathyroid adenoma. Parathyroid adenoma is a benign neoplasm derived from parathyroid parenchymal cells. The parathyroid glands play a key role in calcium homeostasis. Parathyroid adenomas are responsible for hyperparathyroidism in 30 to 90 % of the cases [1]. Hyperparathyroidism can present with a multitude of symptoms. Some as innocuous as generalized weakness & some which may involve pain such as renal stones. Even psychiatric manifestations have been described in hyperparathyroidism. Hence a patient with hyperparathyroidism could seek the help of various specialists in medicine ranging from endocrinologists to urologists. Cohesion, exchange of ideas & a patient centric approach is essential in management of such cases. The old adage ‘too many cooks spoil broth’ is a reminder that conflict & exertion of superiority of one branch to another will not augur good for patient. Our case report is an illustration of how teamwork and an interdisciplinary approach between different branches of medicine will stand patient in good stead [2].
Case presentation
A 74-year-old man presented to the surgeon with nephrolithiasis, weakness & fatigue. An endocrinologist’s opinion was sought. It came to light through radionuclide scan & parathormone (PTH) testing that the patient harboured a parathyroid adenoma. A diagnosis of primary hyperparathyroidism was established. The surgeon had planned for left lower parathyoidectomy in his hospital & testing for intraoperative PTH levels. A drop in the IOPTH > 50 % is considered as successful excision of the parathyroid glands [3,4,5]. However, the hospital laboratory did not have the facility to test of intraoperative PTH levels. The clinical team came in touch with the laboratory team of Apollo diagnostics. The reference laboratory of Apollo diagnostics was situated 20 km away from location where surgery was to take place.
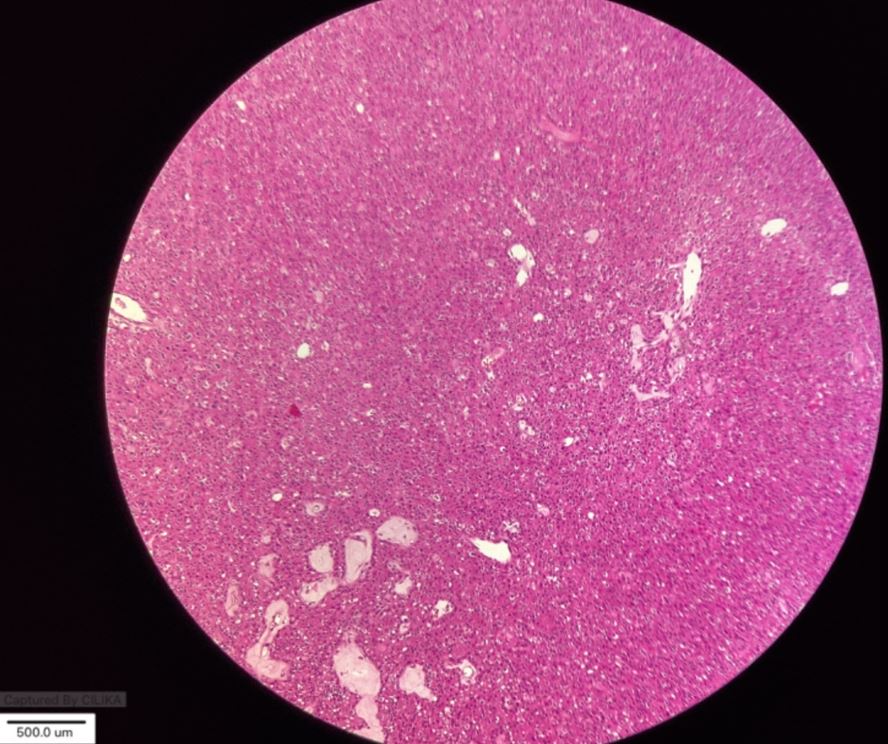
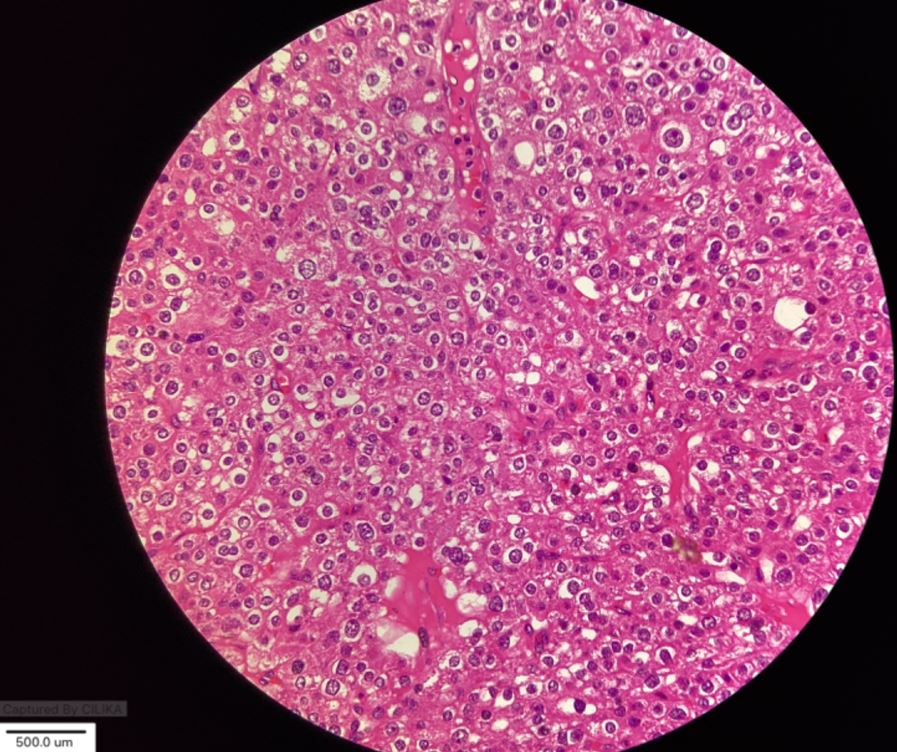
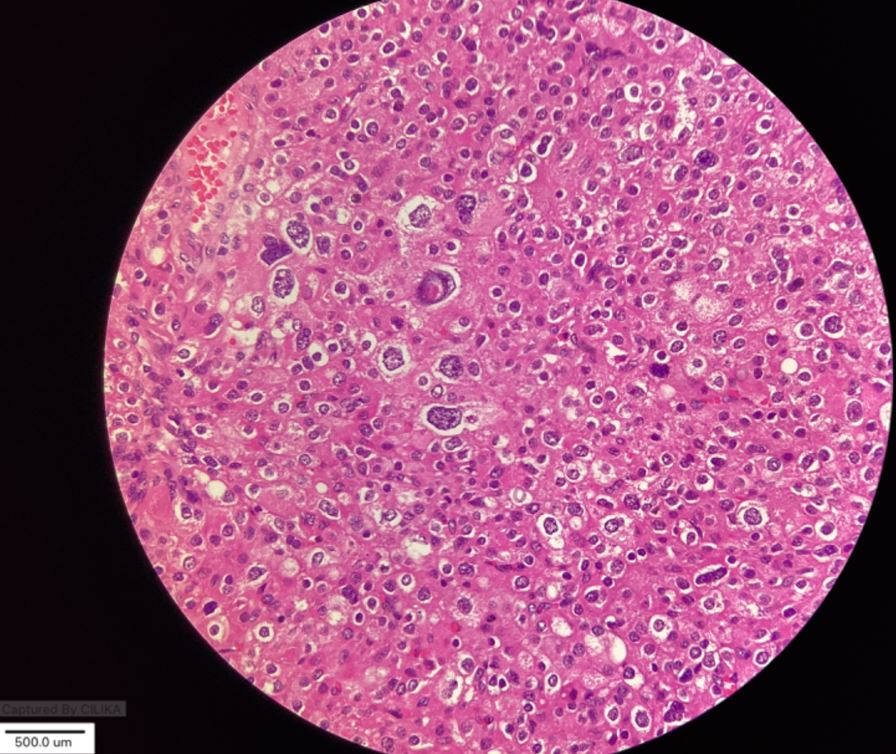
However, with meticulous planning & exchange of ideas, it was decided that surgery be performed in the early hours of a Sunday morning. The early hours of Sunday were chosen to avoid the brunt of city’s traffic. The base line as well as IOPTH samples were transported to the testing facility by ambulance within an hours’ time & samples were tested after all the pre-requisites for sample testing such as QC checks were passed. The results were satisfactory as drop in PTH level was > 50 % The excised glands were subjected to histopathological study & the diagnosis of parathyroid adenoma was confirmed.
Discussion
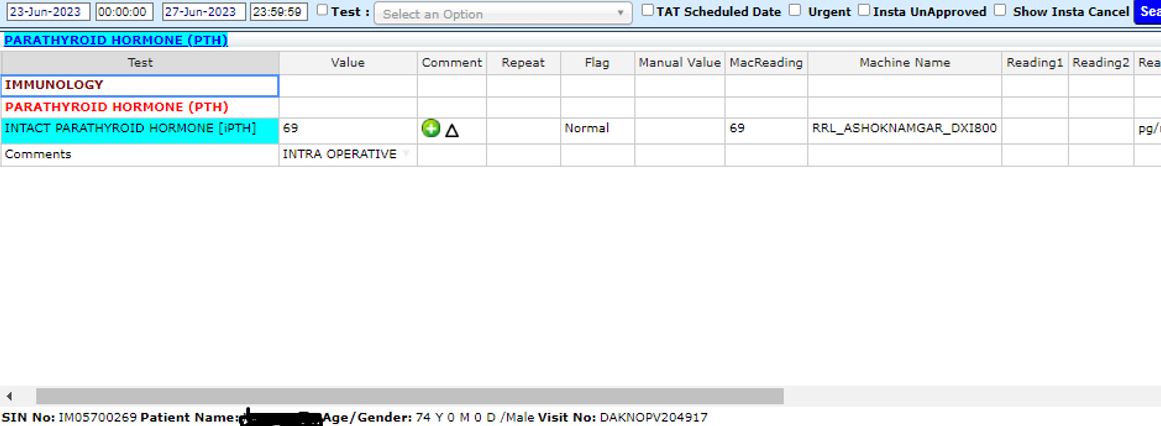
Parathyroid adenomas are the commonest cause of primary hyperparathyroidism & account for 85 to 95 % of the cases [1,6]. Patients with parathyroid adenoma can present with bone disease, nephrolithiasis, gastrointestinal disturbances, central nervous system alterations & cardiac manifestations. Grossly, parathyroid adenomas tend to be located in the lower glands > upper glands & the same held true in our patient. However, despite many attempts the best imaging technique for localizing abnormal parathyroid tissue, the best “technique” for successful localization of abnormal parathyroid glands is an experienced surgeon. The patient on whom left lower parathyoidectomy was done presented with nephrolithiasis, weakness & fatigue. The radionuclide scan as well as PTH levels of the patient suggested primary hyperparathyroidism & the cause was ascribed to parathyroid adenoma. It is worth recalling that parathyroid adenomas are associated with MEN (multiple endocrine neoplasia) syndromes. Intraoperative estimation of PTH is termed “biochemical frozen section. The expertise of the biochemist cannot be understated & thorough scrutiny of pre-requisites such as quality control (QC), analyser maintenance & sample acceptability criteria were given due attention prior to the testing of the samples. On the basis of the Irvin criterion, an intraoperative PTH drop >50% from the highest either pre incision or pre excision level after parathyroid excision was considered a surgical success. Both baseline & intraoperative PTH samples were collected from the patient & were transported to the testing facility within 1 hour. The percentage difference between pre-operative & intraoperative PTH levels was 165 %, which satisfied Irvin criterion [1,5,6].

Picture 1: Pre-operative PTH levels as shown in the laboratory LIS