Introduction
The main manifestation present in Apert Syndrome (AS) and Crouzon Syndrome (CS) is craniosynostosis. Craniosynostosis is a condition of early fusion of the skull bones (Bhoj & Zackai, 2021; Lu et al., 2020). The early sutural fusion impairs skull growth and gives rise to craniofacial dysmorphism in the AS and CS (Das & Munshi, 2018; Lu et al., 2021). AS is one of the complex syndromes that causes craniosynostosis and hand and foot fusions. It was first described by Eugene Apert in 1842. It is also known as acrocephalosyndactyly (Junaid et al., 2023; Ko, 2016; Sawh-Martinez & Steinbacher, 2019). Other than craniosynostosis, craniofacial dysmorphism, visual impairments, cleft palate, and hearing loss are found in AS. The bilateral coronal synostosis is most frequently found in the AS (Alsaeed et al., 2023; Kumari et al., 2023; Massimi et al., 2019). Other metopic, lambdoid, and sagittal suture fusions are also found rarely in AS patients. There is a known genetic cause for the early closure of the cranial sutures in patients with AS (Choudhary et al., 2023; Faasse & Mathijssen, 2023; Koca, 2016; Tan & Mankad, 2018; Timberlake et al., 2023).
In 1912 Octave Crouzon first identified Crouzon syndrome (CS) (Al-Namnam et al., 2019; Balyen et al., 2017). This condition has complete penetrance and variable expressivity. CS is an autosomal dominant disorder, with common features such as the long face, proptosis prominent jaw, hypertelorism, exophthalmos, maxillary hypoplasia, hearing loss, and beaked nose, along with synostosis of coronal, sagittal, and lambdoid sutures (Motch Perrine et al., 2017; Rostamzad et al., 2022; Shlobin et al., 2022; Taylor & Bartlett, 2017; Tønne et al., 2020). The prevalence rate of AS has been estimated to be between 1/65,000 new-borns, and CS estimated as 1/25000 new-borns, without prediction by gender (Munarriz et al., 2020; Munib et al., 2023). AS and CS is associated with advanced paternal age, maternal infections, maternal drug consumption, and cranial inflammatory process (Fernandes et al., 2016; Kyprianou & Chatzigianni, 2018; Lu et al., 2019; Sakamoto et al., 2021). More than 98% of patients of AS and CS are caused by Fibroblast Growth Factor (FGFR2) gene-specific missense pathogenic mutations at chromosome 10q25-10q26 (Azoury et al., 2017; Morice et al., 2020). The FGFR belongs to the family of mitogenic signaling molecules that play an important role in the control of cell proliferation and survival (Luong et al., 2019; Ma et al., 2023).
AS and CS Patients fibroblasts are not able to produce the essential fibrous material in several craniofacial tissues, including bone sutures and cartilage, and during odontoblast formation and regeneration (Di Rocco et al., 2023; Elarjani et al., 2021; Hoshino et al., 2023). Most of the variations are missense variations in theFGFR2leading to craniofacial dysmorphism, and hand and feet malformations. Several syndromes are associated withthe FGFR2gene. These phenotypes also include Antley Bixler syndrome, Beare Stevenson syndrome with cutis gyrata, Pfeiffer syndrome, Jackson Weiss syndrome, and Saethre Chotzen syndrome clinically classified as per additional digital anomalies, skin furrows and skeletal bowing and synostoses (Kiziltug et al., 2023; Pinto et al., 2023; Stanton et al., 2022).
In AS and CS patients the most commonly explored features are asymmetry in mandibular width, height and length, dental arch dimensions, and cranial suture fusion. In this review, we discuss theFGFR2gene-related craniofacial dysmorphism of rare syndromes which include AS and CS.This is the first systematic review focused on craniofacial dysmorphism of two syndromes associated with oneFGFR2gene. This meta-analysis aims at better understanding the craniofacial dysmorphism in AS and CS by exploring the previously published scientific literature.
Material and Methods
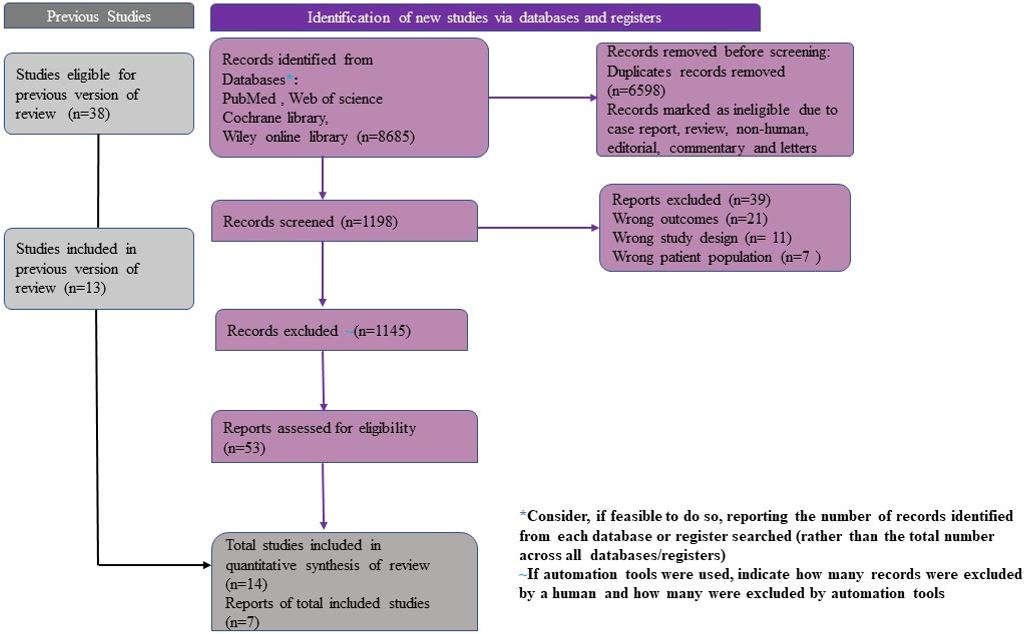
This systematic review was carried out according to the preferred reporting methods for systematic reviews and meta-analysis (PRISMA 2020) guidelines [Table S1] (Page et al., 2021). The protocol was submitted to the International Prospective Register of Systematic Reviews CRD42023395454 accessed 11 February 2023.
Search Eligibility
Search includes peer-reviewed journals and publications that have full-text articles on AS and CS being discussed. Among the different types of research that have been ruled out are animal mice studies, clinical case reports, pilot studies, bibliographic reviews, book chapters, and systematic reviews. The four main steps included in selecting the article are Identification, Screening, Eligibility, and Inclusion.
There were case-control, cross-sectional, cohort studies that compared the Cephalometric CT scan, and radiographs of patients of AS, CS, and non-syndromic patients. Most studies discussed different aspects like maxillary, and mandibular dysmorphism, dental arch asymmetry, and cranial vault dysmorphism. All research papers that matched inclusion criteria were included. Researchers worked independently and reviewed title and abstract of all records to select all relevant studies and any discrepancies over results were resolved.
PICO Search strategy
The following numbers of electronic databases were used for search: PubMed, Cochrane, Medline, Web of Science from date of publication 2000 January to 2023 January [Table S3]. The main search terms used were craniofacial OR craniosynostosis (Apert syndrome) OR (craniofacial dysmorphism) AND (Crouzon syndrome) OR (craniofacial dysmorphism) AND (((Craniosynostosis [Title/Abstract])) OR (Cranium [Title/Abstract])) OR (FGFR2[Title/Abstract]).
Inclusion /exclusion criteria
The systematic review and meta-analysis inclusion criteria: studies on humans, papers written in English, children with descriptive studies such as case reports, case series, and randomized controlled trials, furthermore cohort studies, and case-control studies of Apert and Crouzon syndrome with craniofacial dysmorphism were included. This meta-analysis was not made on ethnicity or gender basis. Exclusion criteria: The cross-sectional studies, editorial, systematic reviews, and meta-analyses were excluded. The enrolled patients who had pathological fractures were excluded.