Introduction
Staphylococcus aureus is primarily responsible for the persistent infections in chronic wounds[1].According to the results of a meta-analysis, the pooled prevalence of MRSA in India between 2015 to 2020 is 37%. There has been a gradual increase in the prevalence rate of MRSA over a period of time. Highest prevalence of MRSA was found to be 55% in Jammu and Kashmir.In all zones of India, there is uniform reporting of prevalence rate[2].
World Health Organization (WHO) has emphasized that MRSA is one of the high priority pathogen among multidrug-resistant organisms[3]. It is capable of producing recurrent infections in wound tissue. This property is attributed to its sturdy biofilm formation. The manifestations range from a simple skin infection to fatal bacteraemia. The pathogen is generally found in urine, blood, sputum and other body fluids. However, it is highly prevalent in wounds[4].
A case control study has arrived to the conclusion that prolonged hospitalization and surgical procedures are risk factors for MRSA infection[5]. Maha Megarajanga Thailam is a unique preparation used externally as well as internally .This formulation includes castor oil as a base added with more than 180 plant parts and minerals. Vaidyar Sachidananda Swamigal had this unique preparation in his clinical practice for the past 40 years . This formulation is prepared preferably during the Munpani kalam (margazhi, thai-Mid January to Mid-February) and collection of the raw materials will be done in month karthigai (Mid November to mid-December).Finished product will be stored in a mud vessel and sealed properly and buried under earth for one mandalam -48 days (Bhoomi Pudam)[6].
It has got unique therapeutic values against skin lacerations, burns, contusions, and diabetic wounds. A case report signifies that Maha Megarajanga Thailam can be effectively used as an adjunctive treatment in diabetic foot ulcer along with the management of appropriate antidiabetic strategy[7]. From GC–MS analysis, it is evident that specific molecules like Squalene, methylsulfanyl, Caryophyllene, Vaccenic acid, and Ricinoleic acid in addition to fatty esters and fatty acids are accountable for the healing property. Further, compounds such as Eugenol, Squalene present improves medication absorption from skin and act against bacteria, fungi, angiogenesis, tumours respectively. Ricinoloeic acid is the most abundant compound found in MMRT and it’s esters are primarily used in modern science as emulsion stabilizers and skin conditioners[8].
Methodology
In the present study, agar well diffusion assay and broth dilution assays were followed to assess the antibacterial activity of the experimental samples MT and MMRT. The following bacterial cultures were chosen for the study: Pseudomonas aeruginosa- ATCC 27853TM; Escherichia coli - ATCC 25922TM; Staphylococcus aureus- ATCC 25923 TM; MRSA (Methicillin-resistant Staphylococcus aureus) - isolated from blood culture. Their storage and standardisation were carried out as per NABL norms.
Agar well diffusion method:
Before proceeding to the agar well diffusion study, the test organisms were sub-cultured onto fresh plates of Mueller–Hinton agar (Hi Media laboratories, India) for 24 h at 37 °C. Colonies from these plates were suspended in Mueller–Hinton broth to a turbidity matching 0.5 McFarland standard (1.5 X 108 CFU/mL) and were incubated appropriately as specified for each organism for a period of 18–24 h (9).
Agar well diffusion assay was carried out(10).In brief, 100 μL of standardized inoculum of each test bacterium was spread onto sterile Muller–Hinton Agar. A 9 mm sterile polystyrene tip was used to make the well. Each well was filled with the defined volumes of MMRT (25, 50 and 100 µL, 130 µl, 150 µl) and then incubated at 37 C for 24 h. Triplicates were prepared for each sample. The experimental sample having antimicrobial activity inhibits microbial growth and formed the clear zones around the well. The zone of inhibition was measured in millimetres (11). The percentage activities of MMRT were calculated against standard drug (mupirocin) which were considered 100%.
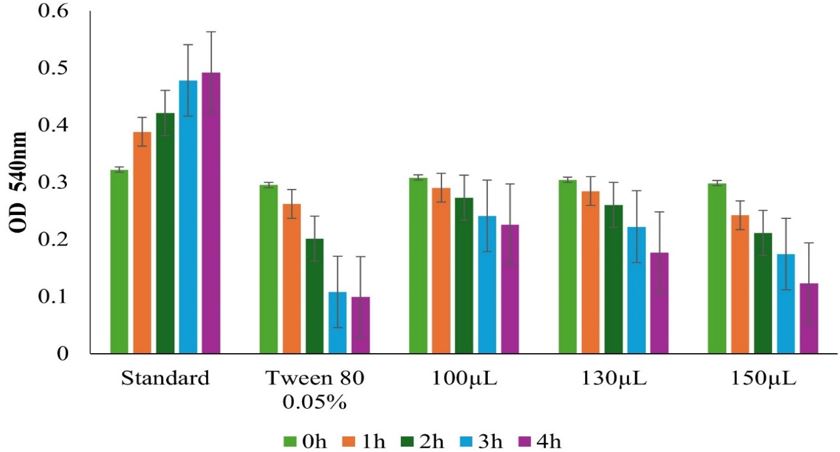
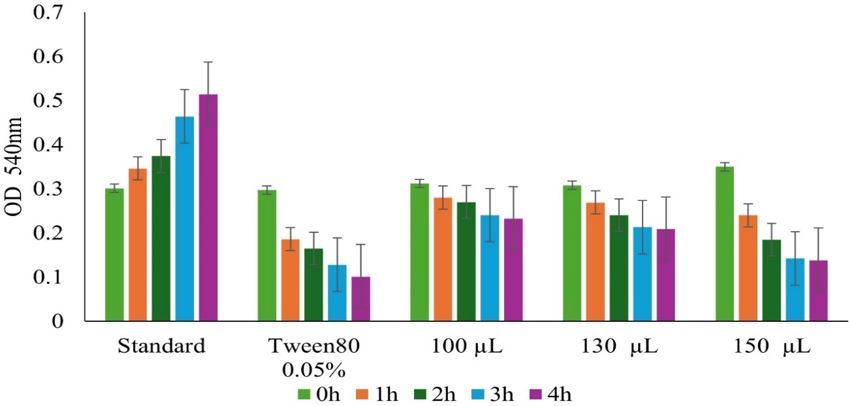
Broth dilution method:
To assess the antibacterial activity using the broth dilution method, experimental samples were emulsified with Tween 80. Tween 80 (0.05%)used as a control sample. Three different volumes of MMRT (100 µL, 130 µl, 150 µl) were chosen for the study. The aliquot of the emulsion was indented with nutrient broth and the final volume of the culture broth was kept at 1.5 ml. To each tube, 0.5ml of test bacterial culture (overnight grown) was indented and incubated at 37 0C for 12 hours. The test tubes were then subjected to serial dilution to the final concentration of 10-7 and plating was done and followed by incubation, the number of colonies shown growth in each dilution was calculated accordingly.(12)
Results and Discussion
aureus and MRSA strains were found to be susceptible to Maha Megarajanga thailam though in different concentrations. MMRT shows that bacterial growth is effectively inhibited at 150 μL concentration. Formation of zone of inhibition started at a concentration of 100μL of MMRT. Table 1 illustrates the size of zone of inhibition formed by MMRT in varying concentrations. The highest antibacterial activity was recorded against S. aureus and MRSA at a concentration of 150 μL. The least activity was recorded against Pseudomonas & E.coli.(Table 1).
Table 1: Antimicrobial properties of MMRT- using Agar well diffusion method
There was a significant variation in zone of inhibition with respect to Gram-negative and Gram-positive organisms. E. coli (ATCC 25922TM) showed moderate sensitivity of 9.8 ± 0.1 mm towards MMRT samples when compared to the standard drug Mupirocin (5µg).The zone of inhibition of the standard was found to be 22 ± 2 mm irrespective of increasing concentration. Zone of inhibition of P. aeruoginosa (ATCC 27853 TM) was measured as 9.4 ± 0.2 mm indicating that it has only mild to moderate sensitivity towards MMRT.