Relationship between Serum Uric acid and BMI in Pre Diabetics and Type II Diabetics in Rural Population – A Pilot Study
Srikanth S.1*, Lavanya Y.2, Sushma K.3
1* Sajja Srikanth, Professor, Department of Physiology, Dr. PSIMS & RF, Chinnavutapalli, Andhra Pradesh, India.
2 Y Lavanya, Assistant Professor, Department of Physiology, Dr. PSIMS & RF, Chinnavutapalli, Andhra Pradesh, India.
3 K Sushma, II M.B.B.S., Department of Physiology, Dr. PSIMS & RF, Chinnavutapalli, Andhra Pradesh, India.
Background & Objectives: People with pre-diabetes may have impaired fasting glucose (IFG) or impaired glucose tolerance (IGT). Some people may have both IFG and IGT. Uric acid can act as a prooxidant and may be a marker of oxidative stress, but it may also have a therapeutic role as an antioxidant. Hyperuricemia has been found to be associated with obesity and insulin resistance. Materials & Methods: The study was conducted in 100 male subjects in the age range 30-50 years. The questionnaire with questions on demographic data, seafood consumption, drinking and smoking information, personal and family history of diabetes and gout, previous history of hypertension, cardiovascular disease was taken. Height & Weight of the subjects was measured. BMI was then calculated. BP was recorded. Serum Uric acid was measured using Uricase-Trinder –Endpoint ; Erba Diagnostics ). For the diagnosis of pre diabetes the WHO (1999) criteria was used. In this study the enzymatic glucose oxidase - peroxidase (GOD – POD ; Erba Diagnostics) was used for estimation of blood glucose level. Results: From the present hospital based cross sectional study, we observed a significant increase in the serum uric acid levels in prediabetics when compared with the control & non diabetic subjects. Conclusion: Uric acid may perform the role of marker for deterioration of glucose metabolism. Pre-diabetics were at higher risk of developing uric acid related complications
Keywords: Atherosclerosis, Body Mass Index, Diabetes, Hyperuricemia, Insulin Resistance, Prediabetes
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Physiology, Dr. PSIMS & RF, Chinnavutapalli, Andhra Pradesh, India. Email:  |
Sajja Srikanth, Y Lavanya, K Sushma, Relationship between Serum Uric acid and BMI in Pre Diabetics and Type II Diabetics in Rural Population – A Pilot Study. Biomed Rev J Basic Appl Med Sci. 2014;1(2):36-42. Available From https://www.biomedicalreview.in/relationship-between-serum-uric-acid-bmi-pre-diabetics-type-ii-diabetics-rural-research-article |
 |
 ©
© 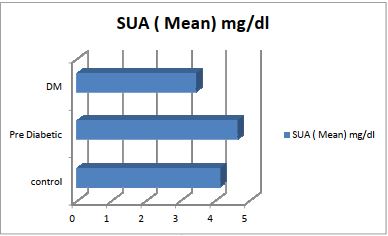 Fig 1: Graph showing Serum Uric Acid in different
Fig 1: Graph showing Serum Uric Acid in different